Carevia overview
Overview
Carevia is a concept exploration developed through rapid prototyping and vibe-coding to examine how patients and caregivers can better prepare for high-stakes medical conversations. The experience focuses on decision preparation, organizing and selectively sharing information with clarity and control.
Rather than automating diagnosis or interpreting medical data, Carevia is positioned around the moment before the appointment, when preparation matters most and clinical liability is lowest.
My Role
On this concept exploration, I owned:
Problem framing and research synthesis
Experience definition and interaction design
Feasibility and scope decisions
Risk and trust tradeoffs
The Problem
Patients and caregivers coordinate care across fragmented portals, providers, and documents, often under time pressure and emotional stress.
Existing portals store records but offer limited support for:
Preparation before appointments
Caregiver collaboration
Selective information sharing
In practice, people rely on screenshots, PDFs, and improvised workflows, increasing confusion and privacy exposure.
Research synthesis revealed that preparation, not interpretation, is the most failure-prone moment in the care journey, especially in multi-provider chronic care households.
Strategy: Decision Preparation, Not Automation
Carevia is intentionally positioned around preparation rather than clinical judgment.
Automated interpretation introduces:
Clinical liability
Hallucination risk
False reassurance
Regulatory exposure
Preparation supports clarity without assuming medical authority.
Early exploration included AI summaries and longitudinal dashboards. Both were intentionally cut after risk modeling revealed governance complexity beyond MVP tolerance.
Carevia consolidates information around a specific moment of need and gives users explicit control over review and sharing, prioritizing trust over technical novelty.
Why Appointment Preparation Became the Anchor
Appointments are:
Emotionally intense
Cognitively overloaded
Time-bound
Error-prone
Rather than build dashboards, analytics, or scheduling systems, I centered the MVP on this constrained, high-value moment where clarity matters most and risk is lowest.
This made the concept focused, defensible, and adoption-ready.
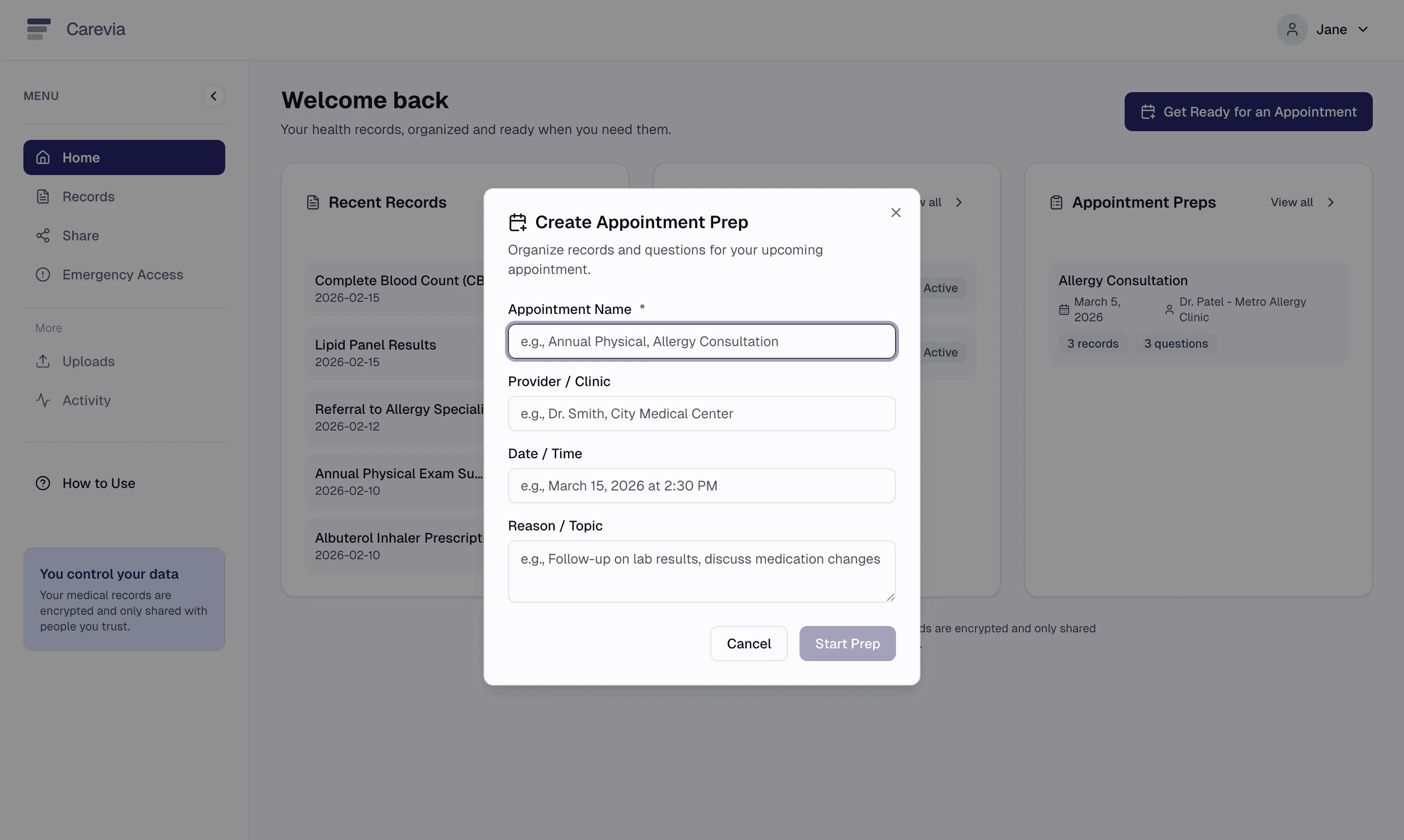
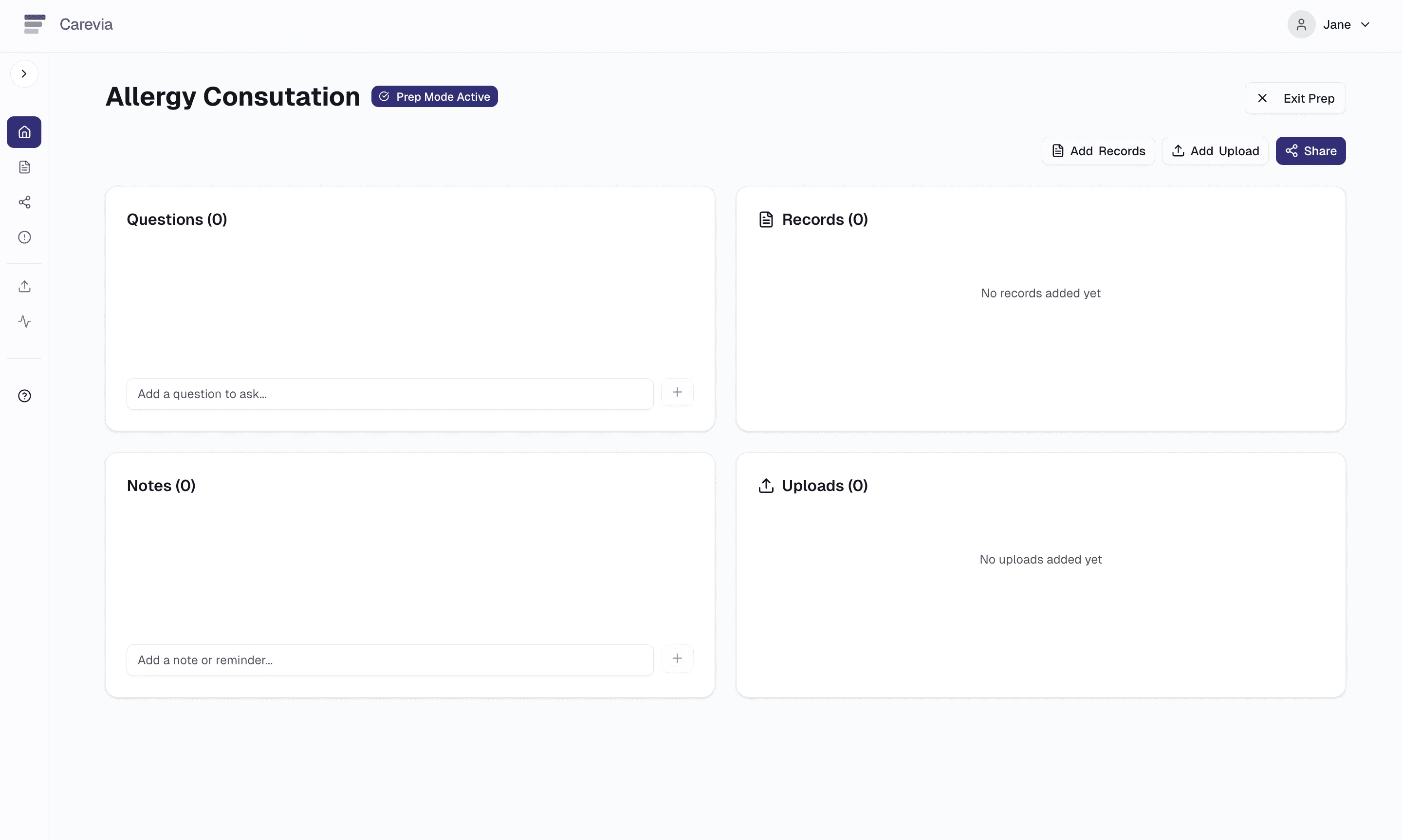
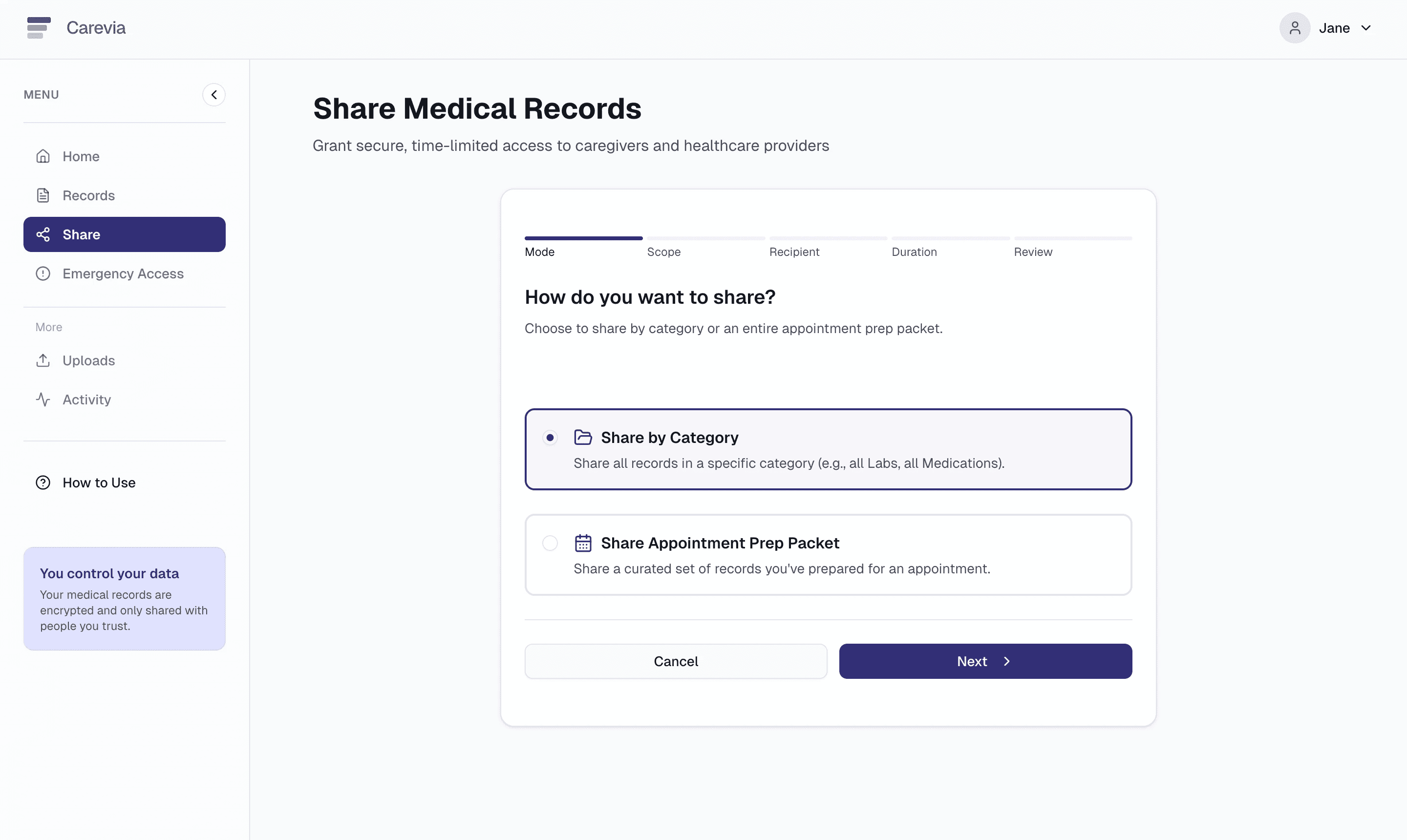
Appointment Preparation Flow
Appointments function as lightweight preparation containers, not calendar events.
Each container supports:
Adding documents (uploads, screenshots, PDFs)
Attaching notes and questions
Curating what will be shared and with whom
The primary entry point, “Get Ready for an Appointment,” reinforces a task-based mental model rather than reliance on external scheduling systems.
Sharing is structured as a controlled set with role-based, time-limited access.
Explore Appointment Prep
Swipe →

Carevia landing page
Appointment Prep 2
Appointment Prep 3

Appointment Prep 4
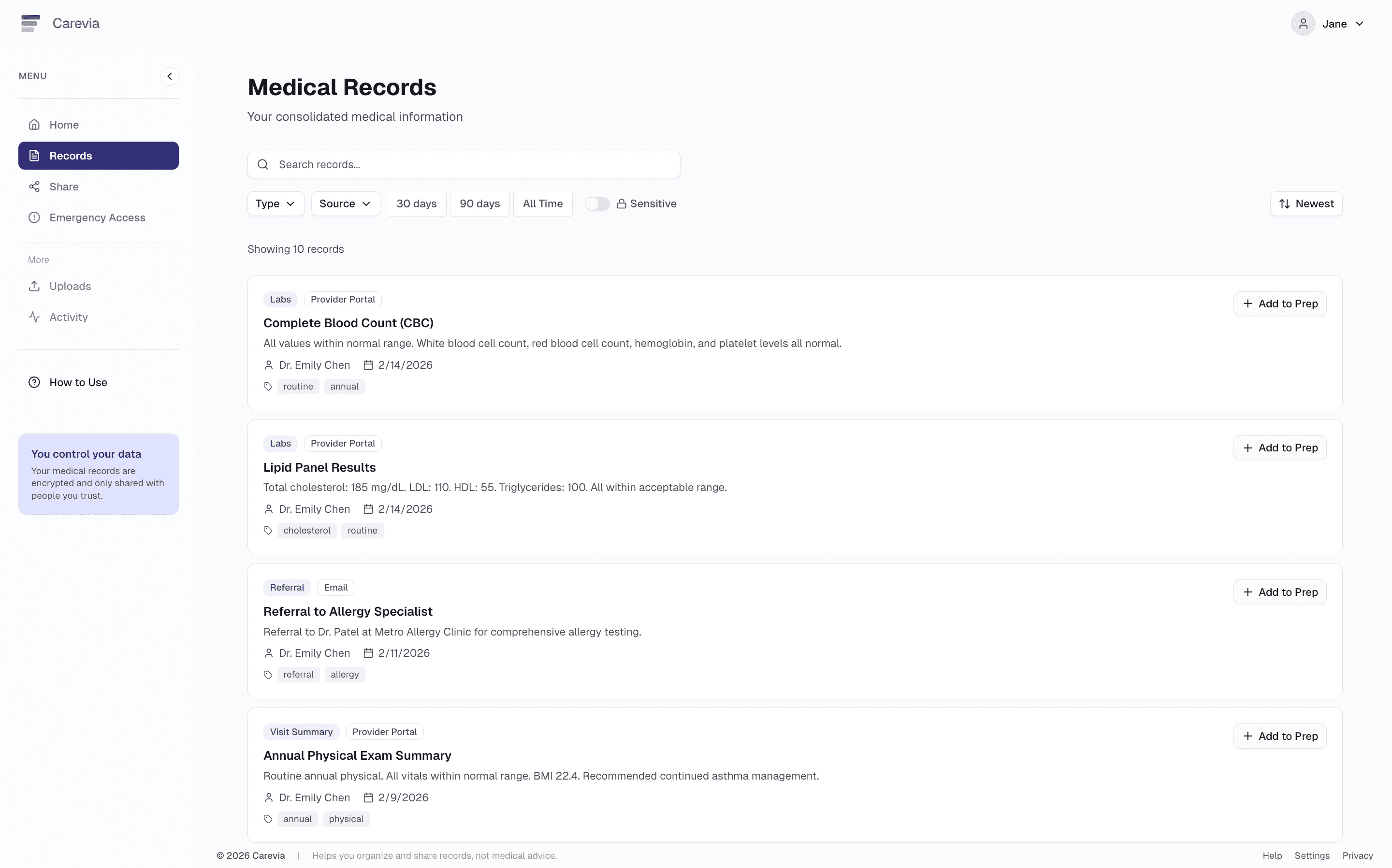
Medical records section
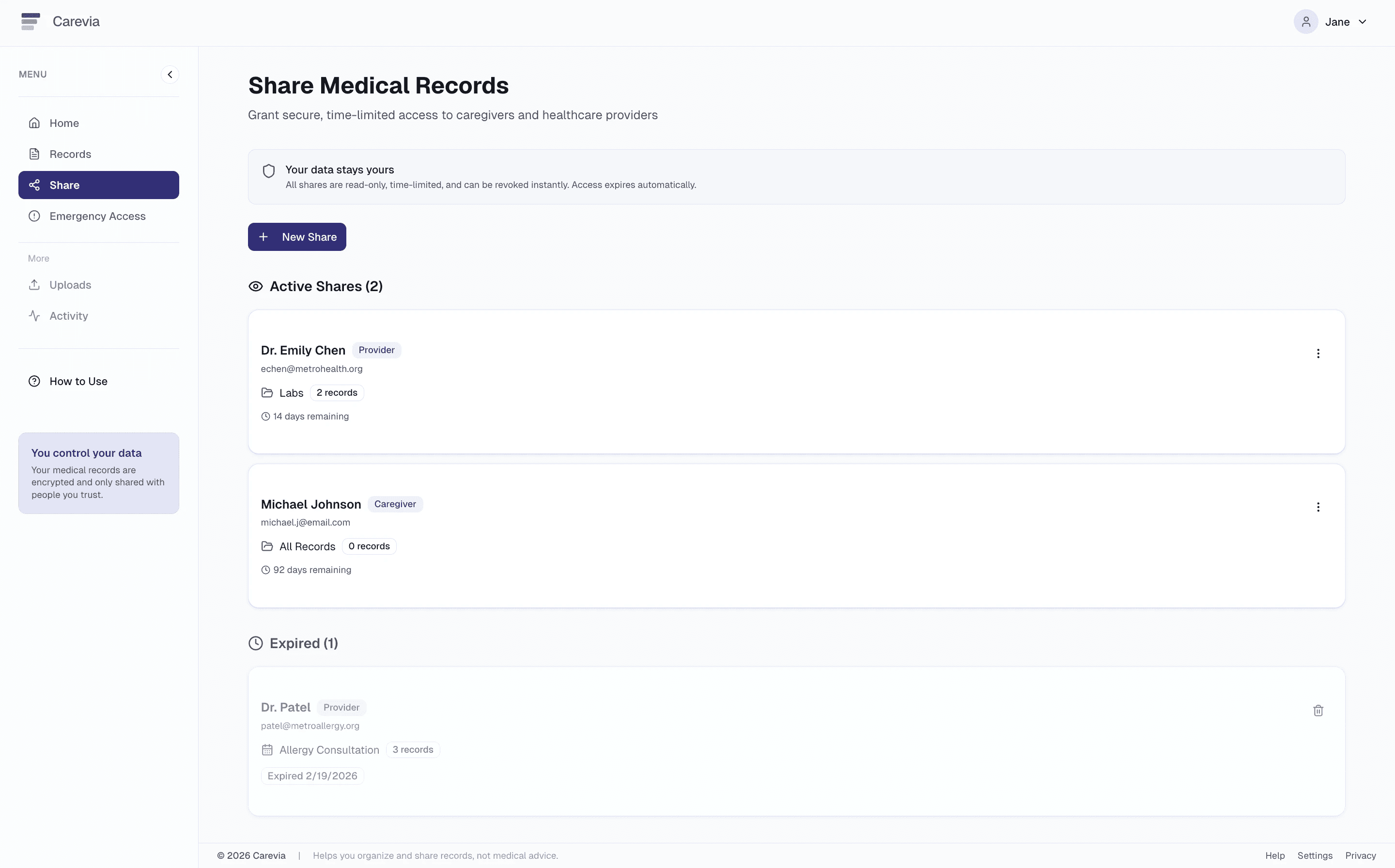
Share section
Share step 2
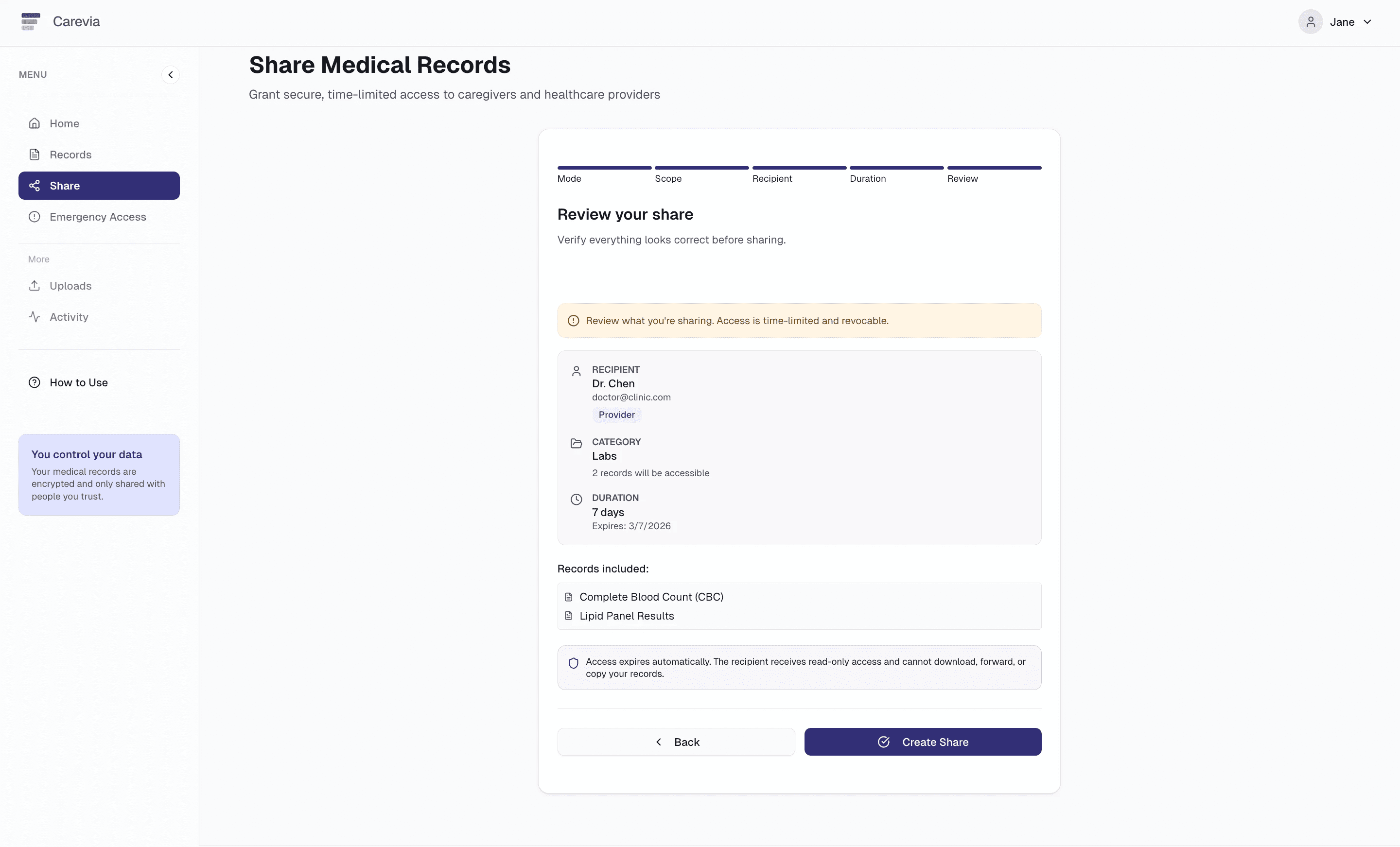
Share step 6

Share confirmation

Emergency Access
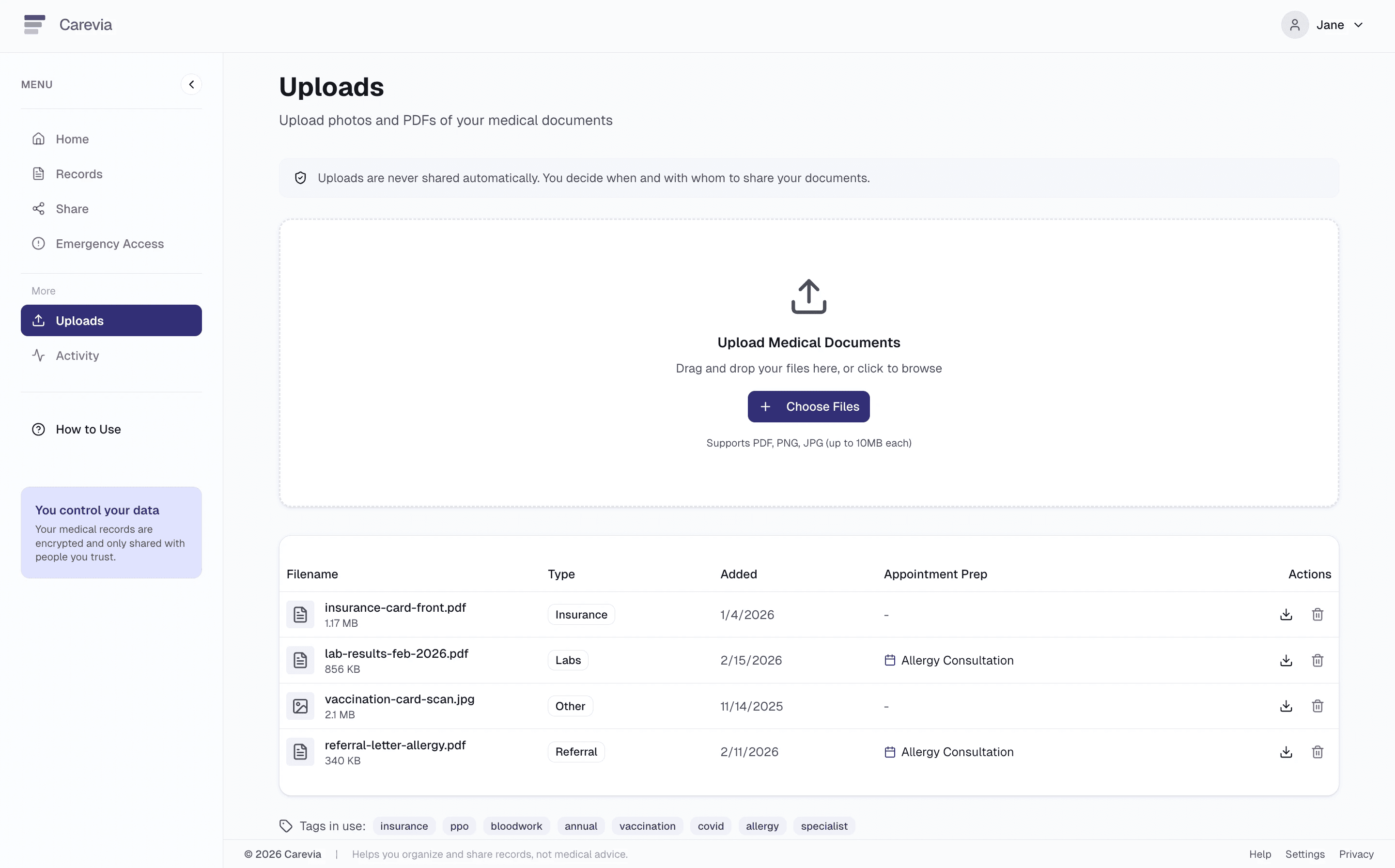
Uploads
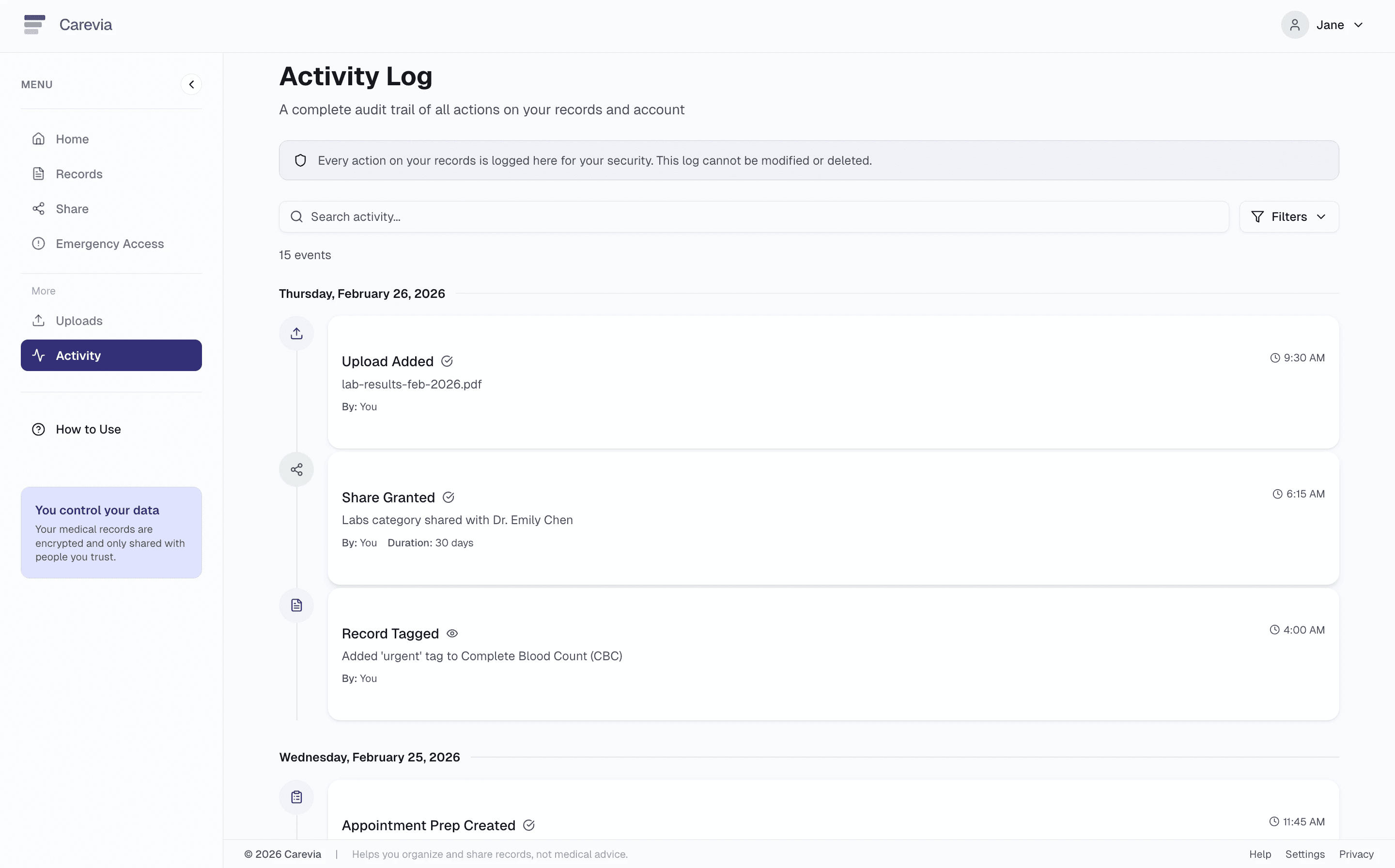
Activity Log

How to guide
Risk Mitigation by Design
The experience intentionally avoids:
Diagnosis or recommendations
Predictive outputs
Automated interpretation of records
EHR write-back
Persistent raw medical record storage
Restraint is deliberate, not a technical limitation.
In healthcare, exclusion is often a leadership decision.
Human-in-the-Loop Design
Carevia keeps people fully in control:
Nothing is shared by default
All actions require confirmation
Access is explicit and revocable
The system is designed to fail safely. Users can remove or replace information at any time.
Relationship to Health Systems
Carevia complements existing patient portals rather than replacing them.
It:
Lives upstream of clinical systems
Requires no clinician workflow change
Integrates through user-managed exports
Avoids EHR write-back risk
This reduces procurement friction and respects real-world integration constraints.
Leadership & Organizational Impact
The core leadership decisions on this project were about what not to build.
Shifting from AI-driven interpretation to decision preparation was a deliberate scope call, not a technical limitation. It produced a lower-liability entry point with clearer adoption pathways. Defining explicit product boundaries upfront, no diagnosis, no predictive outputs, no EHR write-back, meant every subsequent design decision had a clear guardrail to work within.
Anchoring the MVP on appointment preparation rather than
building dashboards or analytics kept the concept focused and defensible. The impact hypothesis is measurable: structured preparation reduces downstream coordination friction, a real operational cost in fragmented care systems.
AI accelerated internal prototyping and research synthesis. It was deliberately excluded from clinical-facing functionality. The phase progression is intentional: preparation infrastructure first, constrained summarization second, governed insight layers only after validation and compliance readiness.
In regulated domains, disciplined scope is leadership.
